


Healthcare is undergoing several drastic changes, including workforce reductions, tariffs that may lead to major supply chain disruptions and regulatory upheaval. The inclination of many healthcare systems and hospitals, as they strive for financial survival, will be further reductions in staff or services and tightened budgets. Pharmacy will not be immune to these across-the-board measures.
Despite this, one of the things setting pharmacy apart from many other healthcare departments competing for scarce dollars is our ability to continue to generate considerable revenue. This revenue creation can be relatively immediate and does not require enormous capital investment, as do other centralized/consolidated services. Each task is done just once instead of multiple times at each facility. During these processes, data integrity is greatly improved and data/statistics are consistently generated.
These efforts will be easier if your entire healthcare system uses the same informatics and pharmacy billing systems. But even if you’re not quite there yet, that’s not a deal breaker or reason not to get started with the most important key to this entire endeavor: taking ownership of your facilities’ charge description master (CDM) and working with your informatics and revenue cycle teams to establish an acceptable (and most likely new) format that all facilities will agree meets their needs.
What follows are eight strategies you can use to ensure CDM best practices. For the purposes of this column, let’s assume these practices are going to be implemented in a healthcare system that has 10 hospitals, three ambulatory surgery centers and numerous outpatient clinics, including infusion centers. If the system already had some centralized/consolidated services, then the pharmacy revenue cycle could be an addition; if not, then chosen as a “hub” facility.
![]() Seek out objections and address them. Take the time to listen to why there may be opposition to the final goal of “one for all,” and try to deflect or overcome those issues. Commonly raised issues include timeliness of new CDM additions (they should be rapid so as not to lose charge capabilities) or nomenclature. Not to be facetious, but how many ways could you possibly describe normal saline, NS, Sodium Chloride 0.9%, 0.9% Sodium Chloride, NaCl 0.9%, 0.9% NaCl, and so on?
Seek out objections and address them. Take the time to listen to why there may be opposition to the final goal of “one for all,” and try to deflect or overcome those issues. Commonly raised issues include timeliness of new CDM additions (they should be rapid so as not to lose charge capabilities) or nomenclature. Not to be facetious, but how many ways could you possibly describe normal saline, NS, Sodium Chloride 0.9%, 0.9% Sodium Chloride, NaCl 0.9%, 0.9% NaCl, and so on?

The idea is to follow a mantra of one drug listing maintained by one central location. But here’s a caveat: Shrinking formularies to fit “one listing for all” is never a popular choice, especially if some of the facilities offer special services. Consider having one “master listing” that each hospital has access to but that can be reduced for their hospital as needed. As an example, a pediatric facility has different needs from a geriatric or psychiatric or oncology facility. Also remember that CDM files link the pharmacy drug master (PDM) to what data are sent to the revenue cycle team for subsequent posting to the claim for payment. The tasks at hand are to eliminate inaccuracies and create a defensible pricing strategy. It’s easy to feel discouraged when faced with thousands of line items and few ideas of how to begin.
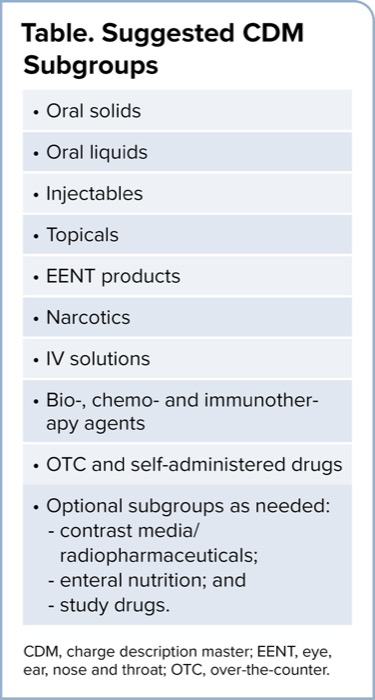
| Table. Suggested CDM Subgroups |
| Oral solids |
| Oral liquids |
| Injectables |
| Topicals |
| EENT products |
| Narcotics |
| IV solutions |
| Bio-, chemo- and immunotherapy agents |
| OTC and self-administered drugs |
Optional subgroups as needed:
|
| CDM, charge description master; EENT, eye, ear, nose and throat; OTC, over-the-counter. |
![]() Determine how your CDM files should look and be used. An important part of that process is to determine, for all facilities and sites of care, how many CDMs with pharmacy items there can be. The answer might be stunning! Identify all places where pharmacy charges originate and eliminate discrepancies between descriptions/charges. Consolidate the multiple CDMs into one database using a marker of some kind (color, code, etc.) to identify which line items came from which facility. Such efforts may be needed to highlight changes that have been made.
Determine how your CDM files should look and be used. An important part of that process is to determine, for all facilities and sites of care, how many CDMs with pharmacy items there can be. The answer might be stunning! Identify all places where pharmacy charges originate and eliminate discrepancies between descriptions/charges. Consolidate the multiple CDMs into one database using a marker of some kind (color, code, etc.) to identify which line items came from which facility. Such efforts may be needed to highlight changes that have been made.
![]() Create subgroups within the CDM. These subgroups form the basis for multiple pricing tiers and allow a variety of price changes per subgroup based on frequency or rate. Rather than having one huge random listing that’s tedious and inflexible, subgroups allow nimble, defensible adjustments. Flexible subgroups can be based on a combination of dosage form and drug category (Table) with an identifier such as a number or letter assigned to each category. Using a sortable database program such as Excel, add this to each line item and sort on the identifier. VoilÀ, your CDM has become more manageable!
Create subgroups within the CDM. These subgroups form the basis for multiple pricing tiers and allow a variety of price changes per subgroup based on frequency or rate. Rather than having one huge random listing that’s tedious and inflexible, subgroups allow nimble, defensible adjustments. Flexible subgroups can be based on a combination of dosage form and drug category (Table) with an identifier such as a number or letter assigned to each category. Using a sortable database program such as Excel, add this to each line item and sort on the identifier. VoilÀ, your CDM has become more manageable!
![]() Shrink excess. Sort each category alphabetically by generic name. Stunned to see how many listings there are for the same drug and how many different prices it may have? Delete as many duplications as possible, remembering that each is linked to the PDM. Deletions may require a PDM/CDM link change as well.
Shrink excess. Sort each category alphabetically by generic name. Stunned to see how many listings there are for the same drug and how many different prices it may have? Delete as many duplications as possible, remembering that each is linked to the PDM. Deletions may require a PDM/CDM link change as well.
![]() Ensure accuracy. The CDM is the link used to tell the patient’s story accurately and completely, and to send claims data to the payor. The accuracy of Healthcare Common Procedure Coding System (HCPCS) and revenue code assignments, as well as inclusion of status indicators (or SIs), is essential. Only a series of codes is sent to the payor, not words describing the drug name and dose. Have you developed a method to validate all billing unit calculations? Is your crosswalk functional? Miscellaneous HCPCS codes must be kept to an absolute minimum. Use them only when a new drug comes to market and has not yet received a unique HCPCS code, and include the National Drug Code, or NDC, number to ensure accurate and representative pricing.
Ensure accuracy. The CDM is the link used to tell the patient’s story accurately and completely, and to send claims data to the payor. The accuracy of Healthcare Common Procedure Coding System (HCPCS) and revenue code assignments, as well as inclusion of status indicators (or SIs), is essential. Only a series of codes is sent to the payor, not words describing the drug name and dose. Have you developed a method to validate all billing unit calculations? Is your crosswalk functional? Miscellaneous HCPCS codes must be kept to an absolute minimum. Use them only when a new drug comes to market and has not yet received a unique HCPCS code, and include the National Drug Code, or NDC, number to ensure accurate and representative pricing.
![]() Examine pricing the CDM. Once again, the mantra is to create a transparent, accurate and defensible pricing strategy. This column is a guide to the thought process as you work through issues at your own facility. There’s no discussion of any specific pricing formula/markup or anything else that could be construed as pricing recommendations. Using a cost-based price markup strategy is common with an added professional fee. The first step could be actual acquisition cost, average wholesale price or wholesale acquisition cost. The database needs to be comprehensive enough to include all products that the pharmacy is responsible for. It’s also important to remember that average sales price tables published by the Centers for Medicare & Medicaid Services are not a viable choice because they are a very limited listing of products paid under the Outpatient Prospective Payment System. Your chosen strategy should be the result of a detailed analysis done in concert with your revenue cycle team. Next comes determining the markup and/or professional fee applicable to each of the categories and subgroups. This step allows you to discontinue flat markups and move to a more defensible strategy of tiered formulas.
Examine pricing the CDM. Once again, the mantra is to create a transparent, accurate and defensible pricing strategy. This column is a guide to the thought process as you work through issues at your own facility. There’s no discussion of any specific pricing formula/markup or anything else that could be construed as pricing recommendations. Using a cost-based price markup strategy is common with an added professional fee. The first step could be actual acquisition cost, average wholesale price or wholesale acquisition cost. The database needs to be comprehensive enough to include all products that the pharmacy is responsible for. It’s also important to remember that average sales price tables published by the Centers for Medicare & Medicaid Services are not a viable choice because they are a very limited listing of products paid under the Outpatient Prospective Payment System. Your chosen strategy should be the result of a detailed analysis done in concert with your revenue cycle team. Next comes determining the markup and/or professional fee applicable to each of the categories and subgroups. This step allows you to discontinue flat markups and move to a more defensible strategy of tiered formulas.
![]() Maintain the CDM. How often are you going to update pricing? Not all subgroups and categories need to have the same frequency of price adjustment. Create a hot-button list of triggers. Examples could be loss of patent exclusivity with subsequent price decreases, contract updates and dramatic price increases.
Maintain the CDM. How often are you going to update pricing? Not all subgroups and categories need to have the same frequency of price adjustment. Create a hot-button list of triggers. Examples could be loss of patent exclusivity with subsequent price decreases, contract updates and dramatic price increases.
![]() Prevent “CDM creep” with insidious additions being requested. After all that work slimming down the document, vigilant attention to detail in keeping it that way is essential. Who’s the “keeper of the CDM”? My vote is for creating a revenue cycle team component in the pharmacy.
Prevent “CDM creep” with insidious additions being requested. After all that work slimming down the document, vigilant attention to detail in keeping it that way is essential. Who’s the “keeper of the CDM”? My vote is for creating a revenue cycle team component in the pharmacy.
More Reimbursement Help!
 | It’s Time to DO(d)GE Data Lapses in 2025 And Beyond Expectations abound when new administrations bring new ideas and new challenges with policy changes! |
 | Here’s How to Properly Bill for Wasted Drugs The fundamental principle in billing for wasted drugs is that some of the medication in specific types of manufacturer single-dose packaging actually is wasted. Of course, there are many other provisions that must be in place for this tricky revenue cycle transaction. |
 | Heads Up: 8 Payment Changes and Challenges in 2025! We’ve entered a new year and a new era with major proposed changes to healthcare. How sturdy are your three pillars of payment? |
 | Please Don’t Stumble On These Payment Basics! Pharmacy has a responsibility for data integrity. It’s an integral, vital part of ensuring that not only is the patient’s story told accurately and completely, but that all claims are processed, submitted and paid. Here are three scenarios depicting instances where working outside the silo to join the revenue cycle/finance team is essential. |
This article is from the May 2025 print issue.