


Since the start of the decade, antibody–drug conjugates (ADCs) have been yielding improved survival rates in patients with gynecologic malignancies (GMs), including a doubling of progression-free survival (PFS). However, as ADCs trend toward “being an important mainstay in gynecologic oncology,” pharmacists must help patients cope with associated toxicities—actions that the profession is well equipped to handle, Cassidy Blaiss, PharmD, BCOP, said during HOPA25, in Portland, Ore.
The first step in managing these patients is to be familiar with the published data on safety and efficacy, noted Dr. Blaiss, a breast and gynecologic oncology pharmacist at the Stephenson Cancer Center of Oklahoma University Health, in Oklahoma City.
In 2021, tisotumab vedotin (Tivdak, Genmab/Pfizer) was the first ADC to be given accelerated approval to treat cervical cancer. In the innovaTV 301 trial that led to full FDA approval, patients treated with tisotumab vedotin had better objective response rates (17.8% vs. 5.2%), median overall survival (OS; 11.5 vs. 9.5 months) and PFS (4.2 vs. 2.9 months) than those who were given chemotherapy (N Engl J Med 2024;391[1]:44-55). Ocular events occurred in 52.8% of patients in the tisotumab vedotin group versus 6.3% in the chemotherapy group, “but most were low grade,” Dr. Blaiss said.
Another key study, the innovaTV 205 trial, established the efficacy of tisotumab vedotin in patients with recurrent or stage IVB cervical cancer with no prior systemic therapy or who had disease progression without anti–programmed death ligand-1 therapy (J Clin Oncol 2023;41[36]:5536-5549). Tisotumab vedotin was given to patients in combination with either bevacizumab, carboplatin or pembrolizumab (Keytruda, Merck). Ocular events again emerged as a noted side effect, with the highest rate occurring in patients treated with tisotumab vedotin and carboplatin (66.7%); 9.1% of those reactions were deemed grade 3, Dr. Blaiss noted.
The next drug to be approved for a GM was mirvetuximab soravtansine-gynx (Elahere, AbbVie), a first-in-class ADC targeting folate receptor alpha, indicated for the treatment of ovarian cancer. In the MIRASOL study (N Engl J Med 2023;389[23]:2162-2174), key favorable outcomes included a greater PFS and OS than investigators’ choice of chemotherapy (5.62 vs. 3.98 months and 16.46 vs. 12.75 months, respectively). However, those clinical gains came with some mostly low-grade ocular toxicities, including blurred vision (40.8%) and dry eyes (28%). Although reversible, “prophylactic and mitigative measures should be adhered to by patients and health care professionals.”
Enhertu Poses a Different Toxicity Challenge
One additional recently approved antibody–drug conjugate, fam-trastuzumab deruxtecan-nxki (Enhertu, Daiichi Sankyo), should be on the radar of oncology pharmacists. Unlike the other ADCs that require particular attention for ocular adverse reactions, fam-trastuzumab deruxtecan-nxki causes pulmonary adverse events that require vigilance, according to Cassidy Blaiss, PharmD, BCOP, a breast and gynecologic oncology pharmacist at the Stephenson Cancer Center of Oklahoma University Health, in Oklahoma City.
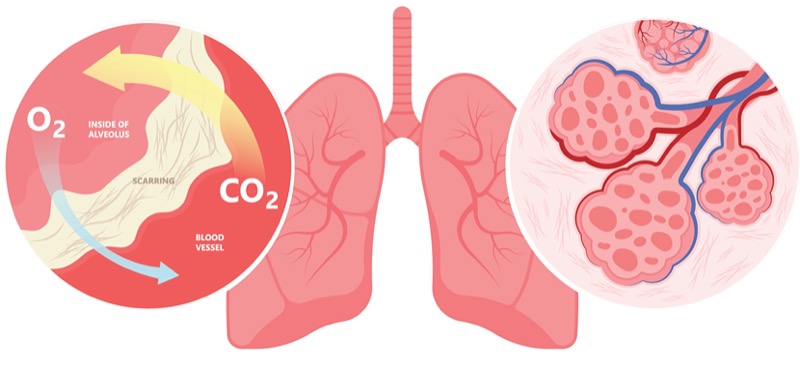
The DESTINY-PanTumor02 study evaluated the use of fam-trastuzumab (T-DXd) with locally advanced/metastatic ovarian, cervical and endometrial cancer (J Clin Oncol 2024;42[1]:47-58). Objective response rate (ORR) was the primary study outcome. Participants with immunohistochemistry (IHC) 3+ malignancies all had a greater than 50% ORR with T-DXd treatment: 84.6%, 75% and 63.6% for endometrial, cervical and ovarian cancer, respectively. T-DXd was granted accelerated FDA approval for HER2 IHC 3+ for any cancer type after prior systemic therapy without a satisfactory alternative based on this trial. However, interstitial lung disease (ILD) occurred at 10.5% across cohorts, and Dr. Blaiss recommended the following steps for managing such cases:
- All patients starting on T-DXd should get a baseline high-resolution CT scan.
- Repeat high-res CT every 12 weeks (or six to nine weeks in patients with baseline respiratory symptoms).
- If grade 1 ILD occurs, Dr. Blaiss recommended that treatment be interrupted. Pharmacists can consider starting steroids at that 0.5-mg/kg dosing and then tapering over four weeks. If ILD is resolved 28 days or less, maintain the dose; if resolved in more than 28 days, reduce one dose level.
- Grade 2 or higher ILD should lead to permanent discontinuation of T-DXd.
To manage patients with at least grade 2 ILD, Dr. Blaiss recommended therapy with prednisone (1 mg/kg per day), with tapering after resolution over at least four weeks. She also warned that patients with ILD of grade 3/4 may require hospital admission and IV steroids (up to 1 g of methylprednisolone), then dropping down to prednisone 1 mg/kg with tapering over at least four weeks.
Dr. Blaiss agreed that “prophylaxis is the best way to manage ocular toxicities for both agents” and recommended lubricating eye drops every day of treatment (at least four times daily), along with the use of steroid drops. She also emphasized the importance of following the guidance provided by manufacturers of each drug, including the use of a slit lamp and visual acuity test before every cycle (1-9) for tisotumab vedotin and every other cycle for the first eight cycles of mirvetuximab soravtansine-gynx. With tisotumab vedotin, vasoconstricting eye drops are recommended just prior to infusion, along with cryotherapy and use of an eye mask during the infusion and a visual acuity test done after completion of therapy.
In an interview with Pharmacy Practice News, Lindsey Chippendale, PharmD, BCOP, a clinical gynecologic oncology pharmacist at the University of Virginia Health, in Charlottesville, agreed that these steps are crucial for ensuring safe treatment with both ADCs. She also explained that educating patients to alert clinicians of emerging ocular toxicities is an important step to “getting in front” of any potential complications.
Despite these measures, ocular adverse events (AEs) are common problems with the ADCs, so Dr. Blaiss offered some additional details on how to manage them:
- Grade 1 AEs in both agents should lead to no changes if steroid prophylaxis is already being used.
- Grade 2 keratitis or keratopathy should lead to treatment being withheld until resolved. Tisotumab vedotin is resumed at the same dose or a dose reduction and discontinued after a second occurrence. Mirvetuximab soravtansine-gynx is resumed at the same dose, and physicians should consider a dose reduction at the second occurrence of a grade 2 event.
- A grade 3 or higher ocular event such as a corneal ulcer, stromal opacity or visual acuity of 20/200 or worse should lead to tisotumab vedotin discontinuation. However, grade 3 AEs with mirvetuximab soravtansine-gynx allow for withholding until improvement and then restarting therapy at a reduced dose.
- Grade 4 events with either agent should lead to permanent discontinuation.
Both Drs. Blaiss and Chippendale noted that there are likely to be several more ADCs approved for GMs in the near future, including sacituzumab govitecan-hziy (Trodelvy, Gilead), which is currently being used off-label to treat endometrial cancer. However, they noted that each ADC is likely to come with its own set of side effects that must be managed actively by pharmacists. Dr. Blaiss concluded that “a careful review of literature and adverse events can help pharmacists stay alert to emerging toxicities.”
The sources reported no relevant financial disclosures.

This article is from the June 2025 print issue.