

Clinical Pharmacy Services and Quality Assurance
Option Care Health
Denver, Colorado
National Institutes of Health
Bethesda, Maryland
Mississippi Baptist Medical Center
Clinical Associate Professor
University of Mississippi School of Pharmacy
Jackson

Parenteral nutrition (PN) is a lifesaving therapy for patients who are unable to meet their nutritional needs via the gastrointestinal tract. PN orders are highly individualized and require precise calculations based on a patient’s clinical status, nutrient requirements, fluid restrictions, and organ function. Formulations include macronutrients (dextrose, amino acids, and lipid injectable emulsions [ILEs]), micronutrients (electrolytes, vitamins, and trace elements), and additives such as famotidine or insulin. Pharmacists play a critical role in evaluating each of these components to prevent complications such as metabolic disturbances, electrolyte imbalances, and component incompatibilities.
There is no centralized database reporting total numbers of PN patients in the United States; however, estimates range from 300,000 to 350,000 hospitalized and 25,000 to 40,000 home infusion PN patients.1,2 The Institute for Safe Medication Practices (ISMP) recognizes PN as a high-alert medication3 due to the risk of causing significant patient harm when errors are made. High-alert therapies require safeguards to reduce the risk for errors, including standardization, improved access to information, clinical decision support, and redundancies such as double-check procedures.
The large number of patients and complexity of PN therapy requires specialized knowledge and competence from pharmacists responsible for reviewing and verifying these orders. PN orders contain dozens of individually dosed components in each custom solution, and 20% to 39% of the time, something within the order requires additional clarification for safe and accurate administration.4 A recent study noted the top 3 pharmacist PN interventions were electrolyte dose clarification, calcium/phosphorus incompatibility, and amino acid dose clarification.5
Each separate component of a PN order has its own clinical rationale, dosing implications, and interaction potential that requires evaluation and validation during order review. Voluntary error reporting to ISMP over a 10-year period separated by stage of the PN use process showed a 20% error rate in the order review step.6 PN-related product shortages are common and may increase the risk for errors. Therefore, it is imperative that pharmacists complete a review of all PN orders to ensure accuracy, completeness, stability, and compatibility.
PN is a complicated therapy that requires thorough order reviews by clinicians with advanced skills. If pharmacists are going to perform those order reviews, they should be given advanced training and their skills validated through ongoing competency assessments for each step in the PN use process.
In recent years, dedicated institutional nutrition support teams have declined, and the responsibility of ensuring safe PN therapy provision has shifted to a shared responsibility between members of the multidisciplinary care team. With this change, the importance of ensuring adequate PN-related training and expertise has become increasingly critical. In addition to staff education and training, standardization of the PN use process, enhanced electronic health record (EHR) functionality, and competency assessment are paramount among all disciplines involved in the PN use process. This article focuses on the skills and competence required for the order review portion of the PN use process.
Characteristics of Competency
Competency is defined as the quality or characteristics of a person that result in effective performance.7 This combination of knowledge, skills, motives, and personal traits ensures a culture of safety. The Table provides a high-level overview of the various competencies that are important for effective PN order review.8
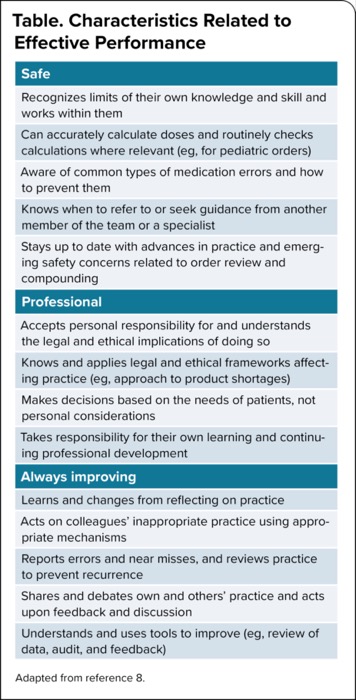
| Table. Characteristics Related to Effective Performance |
| Safe |
|---|
| Recognizes limits of their own knowledge and skill and works within them |
| Can accurately calculate doses and routinely checks calculations where relevant (eg, for pediatric orders) |
| Aware of common types of medication errors and how to prevent them |
| Knows when to refer to or seek guidance from another member of the team or a specialist |
| Stays up to date with advances in practice and emerging safety concerns related to order review and compounding |
| Professional |
| Accepts personal responsibility for and understands the legal and ethical implications of doing so |
| Knows and applies legal and ethical frameworks affecting practice (eg, approach to product shortages) |
| Makes decisions based on the needs of patients, not personal considerations |
| Takes responsibility for their own learning and continuing professional development |
| Always improving |
| Learns and changes from reflecting on practice |
| Acts on colleagues’ inappropriate practice using appropriate mechanisms |
| Reports errors and near misses, and reviews practice to prevent recurrence |
| Shares and debates own and others’ practice and acts upon feedback and discussion |
| Understands and uses tools to improve (eg, review of data, audit, and feedback) |
| Adapted from reference 8. |
The ASPEN Competency Model
The American Society for Parenteral and Enteral Nutrition (ASPEN) has developed a model for standardized competencies and best practices when reviewing PN orders.8 Best practices based on the ASPEN Model include the following:
- Pharmacists hold appropriate licensure or credentials for their profession.
- Pharmacists should be board certified, preferably as nutrition support pharmacy specialists.
- If not board certified in nutrition support:
- pharmacists should have a board-certified nutrition support pharmacy specialist available to provide ongoing training and administer competencies; and
- pharmacists should complete didactic and interactive courses such as ASPEN’s professional development programs (eg, Parenteral Nutrition Order Writing Workshop) or the ASPEN/ASHP Nutrition Support Certificate program.
- Alternatively, an organization may develop an internal program that includes didactic coursework and interactive cases.
An organizational program should include knowledge of all aspects of providing PN therapy, from vascular access to error reporting. Learning should be assessed through a pretest and posttest. The program should include:
- PN indication and vascular access. The indication for PN should be evaluated to ensure appropriateness of the prescription. Once the therapy has been deemed appropriate, vascular access should be considered. The high osmolarity required to meet patient requirements requires central access, and verification of the access placement including distal tip location is important for patient safety.
- Advanced understanding of macro- and micronutrient requirements in various clinical scenarios (eg, age, diagnosis, organ function) including fluid, electrolyte, and acid–base balance.
- Interpretation of physical examination and laboratory findings.
- PN ordering, including dispensing format.
- PN can be dispensed in multiple formats, including:
- a multi-chamber bag (MCB);
- amino acid and dextrose with micronutrients (2-in-1); and
- amino acid, dextrose, and ILE admixture with micronutrients (3-in-1).
- Clarification of the intended formulation is necessary for accurate review of components and administration.
- Total nutrient admixtures, or 3-in-1 formulations, may become unstable if minimum final concentrations of macronutrients are not maintained.
- Each lipid droplet in a 3-in-1 formulation is coated with a negatively charged emulsifying agent to disperse the oil phase into the aqueous phase.
- There are thousands of lipid droplets in every milliliter of lipid emulsion, and each droplet is in a constant state of wanting to coalesce to form larger droplets, potentially leading to an unstable emulsion if not carefully dosed within recommended parameters.
- Manufacturers have provided recommended minimum final concentrations of macronutrients to improve 3-in-1 stability. It is important to utilize the appropriate manufacturer data for the specific formulation being reviewed, as the data are amino acid and lipid specific.
- Micronutrients can also affect stability, particularly trivalent (eg, iron) and divalent (eg, calcium, magnesium) cations. Positively charged cations may disrupt the negatively charged lipid emulsion if not maintained at recommended levels.
- Calcium phosphate solubility is also influenced by the presence of lipids in the admixture, among other factors. Utilizing the correct amino acid product–specific stability curves to assess calcium phosphate insolubility risk for each PN formulation being reviewed is essential to ensure patient safety.
- PN can be dispensed in multiple formats, including:
- Concurrent pharmacotherapy. In addition to the macro- and micronutrient components, non-nutrient medications are sometimes included as part of the PN order. As part of the order review process, the pharmacist needs to determine the safety of including non-nutrient medications in the mixture and how that may affect each component as well as the overall compatibility and stability of the dispensed formulation.
- Monitoring and complication prevention and management.
- Management of component shortages.
- Documentation and tracking of adverse drug reactions and medication, including nutrient products, errors.
A pharmacist should review at least 10 PN orders for the initial competency evaluation and at least 2 for annual competency. Patient case scenarios or actual patients may be reviewed under the supervision of an experienced nutrition support preceptor or trainer. Resources such as the ASPEN Parenteral Nutrition Workbook9 can provide detailed case studies to include in coursework.
PN Order Review Best Practices
To optimize PN patient outcomes, pharmacists should adhere to best practices during the order review process. Utilizing standardized processes and protocols drives safety by reducing variability, minimizing errors in nutrient dosing, and enhancing adherence to evidence-based guidelines.
The PN order data should be standardized, including formulas, formula naming (eg, ILEs or trace element brand names to prevent dosing errors), unit of measure (eg, microgram, millimole), sequence of ingredients, and formulation options (eg, MCB, 2-in-1, 3-in-1). A standardized order format helps reduce the risk for necessary component omission or a unit dosing error. Electronic order entry and transmission are preferred to avoid transcription errors between the EHR and the automated compounding device, or the EHR and an outsourced compounding vendor. If transcription is necessary due to technology limitations, independent double-check processes should always be followed.10
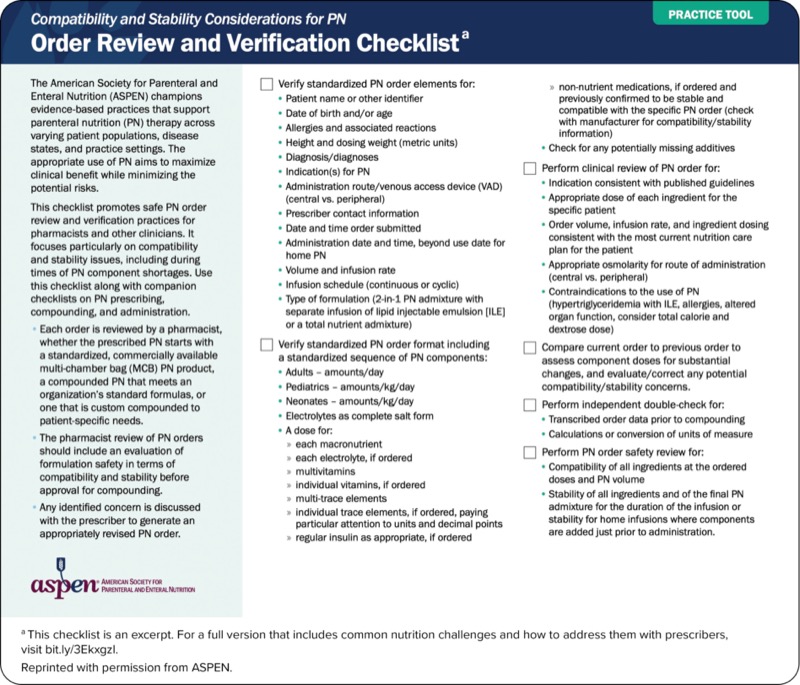
Using a checklist can complement memory and experience to ensure safe PN therapy. ASPEN has developed practice tools that provide safety checklists for each step of the PN use process. The Practice Tool on page 6 provides a standardized safety checklist to ensure best practices with order review and verification.10,11
Conclusion
PN is a necessary and lifesaving therapy. Due to its complex and high-risk nature, PN is prone to dosing errors, and order review and verification are essential components of the PN use process. Pharmacists completing PN order review should have advanced education and training in nutrition support and demonstrate this specialized knowledge and skill through initial and annual competency. ASPEN resources support PN training and competency through program offerings and resources for organizations developing internal programs.
Ms. Figueiroa reported no relevant financial disclosures. Dr. Ayers is a consultant to and/or speaker for American Regent, B. Braun, and Fresenius Kabi. Ms. Monczka is a consultant to Fresenius Kabi.
References
- Guenter P, Blackmer A, Malone A, et al. Update on use of enteral and parenteral nutrition in hospitalized patients with a diagnosis of malnutrition in the United States. Nutr Clin Pract. 2022;37(1):94-101.
- Bezjak J, Szabo K, Tokarski R. Innovative, multidisciplinary management of home parenteral nutrition patients. Infusion J. 2024;3(2):13-16.
- Institute for Safe Medication Practices (ISMP). ISMP List of High-Alert Medications in Acute Care Settings. ISMP; 2024.
- Wischmeyer PE, Klek S, Berger MM, et al. Parenteral nutrition in clinical practice: international challenges and strategies. Am J Health Syst Pharm. 2024;81(suppl 3):S89-S101.
- Kraft MD, Tucker AM, Durfee SM, et al. Parenteral nutrition prescribing and order review safety study: the need for pharmacist intervention. Nutr Clin Pract. 2021;36:480-488.
- Guenter P, Ayers P, Boullata JI, et al. Parenteral nutrition errors and potential errors reported over the past 10 years. Nutr Clin Pract. 2017;32(6):826-830.
- Guenter P, Boullata JI, Ayers P, et al. Standardized competencies for parenteral nutrition prescribing: the American Society for Parenteral and Enteral Nutrition Model. Nutr Clin Pract. 2015;30(4):570-576.
- Boullata JI, Holcombe B, Sacks G, et al. Standardized competencies for parenteral nutrition order review and parenteral nutrition preparation, including compounding: the ASPEN Model. Nutr Clin Pract. 2016;31(4):548-555.
- Cober MP, Blackmer A, Derenski K, et al. ASPEN Parenteral Nutrition Workbook. 2nd ed. American Society for Parenteral and Enteral Nutrition; 2022.
- Ayers P, Adams S, Boullata J, et al. A.S.P.E.N. parenteral nutrition safety consensus recommendations. JPEN J Parenter Enter Nutr. 2014;38(3):296-333.
- ASPEN. (2025, January 6). Compatibility and stability considerations for PN: order review and verification checklist. https://nutritioncare.org/wp-content/uploads/2024/12/PN-Checklist-02-Order-Review.pdf
Copyright © 2025 McMahon Publishing, 545 West 45th Street, New York, NY 10036. Printed in the USA. All rights reserved, including the right of reproduction, in whole or in part, in any form.

Download to read this article in PDF document:![]() Parenteral Nutrition Order Review: Skills and Competencies Required for Success
Parenteral Nutrition Order Review: Skills and Competencies Required for Success