


In response to concerns from health systems and other surveyed organizations, The Joint Commission has made changes to help streamline access to key medication safety information in its Survey Analysis for Evaluating Risk (SAFER) matrix.
The changes began in late January 2025, the organization announced at the ASHP Midyear 2024 Clinical Meeting & Exhibition, in New Orleans.
SAFER, which helps organizations pinpoint Requirements for Improvement (RFIs) needed for preventing harm to patients, now includes a short name and description next to standards and elements of performance (EPs) in the matrix, so that users no longer have to refer to other materials to determine what each one entails. The revised report also will include distinct sections for findings related to immediate threats to health or safety.
“If you have a Medicare deficiency survey, you’ll also have a section for those findings. The findings will be ranked in order from the top of the SAFER matrix, hoping to provide a better idea of where to begin corrections,” said Robert Campbell, PharmD, BCSCP, the senior director, Standards Interpretation, Accreditation Decision Management and Medication Safety, in the Division of Accreditation and Certification Operations at The Joint Commission.
To reduce confusion over what findings must be addressed before a 45-day follow-up visit from the surveyor, only condition-level “parent” tags will be displayed in future Joint Commission survey reports. “The current report format is very confusing, making it difficult to determine a condition from a standard,” Dr. Campbell said. “Moving forward, you will only see the ‘parent’ tag and the ‘child’ tag will be left blank, so you know what will be reviewed when the surveyor returns.”

In most recent Joint Commission medication management surveys, most RFIs were in the moderate or limited category, Dr. Campbell reported. Between Jan. 1, 2023, and June 30, 2024, 1,566 surveys were conducted, with 3,814 RFIs for an average of 2.4 RFIs per survey. Of those, 64.1% were moderate and 10.6% low, while 25.2% were high.
“Out of all of these surveys, the No. 1 high-risk scored item is MM.06.01.01 EP 3, medication administration pre-order verification,” Dr. Campbell said, noting that 42% of surveys included that finding. “The second is MM.05.01.07 EP, the medication compounding process. And when we place these RFIs on the SAFER matrix risk distribution, you’ll see that the highest risk is medication order verification, particularly with regard to medications that are being administered through titration.”
He added that “if you look at an organization’s high-alert medication list, most of the medications that are being titrated are designated as high-risk medications. So by default they become a high-risk finding on the survey report because mismanagement of those medications has been shown to have risk.”
Findings related to titrated medications also appeared in several other high-risk RFIs, including medication order policy (titration medication orders missing required elements) and review/clarify medication order (titration orders written with conflicting clinical end points). “Titration orders continue to be one of our top scoring clinical standards in the hospital program,” Dr. Campbell said (bit.ly/3WDyxaq-PPN).
Range orders are permissible in titration medication orders, he added. “They must include starting doses, titration dose, titration frequency and clinical end points. Clinical end points do not have to be included in the same order, however; they can be provided in a separate order.” (For other RFIs identified in recent Joint Commission medication management surveys, see Table.)
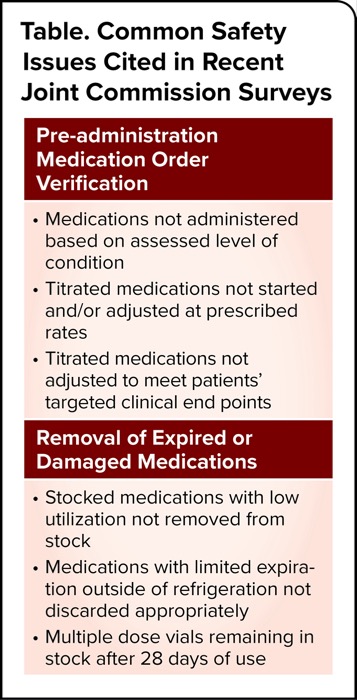
| Table. Common Safety Issues Cited in Recent Joint Commission Surveys |
| Pre-administration Medication Order Verification |
|---|
|
| Removal of Expired or Damaged Medications |
|
Timing Is Key
In a separate interview, Marianne Sevcik, MSN, RN, a former Joint Commission surveyor and the founder of Partnership International, which provides comprehensive mock survey processes for accreditation and regulatory compliance, agreed that titration orders and block charting (sidebar) continue to present challenges in medication management
“Titrations aren’t that complex—and yet they are,” Ms. Sevcik said. “You need a beginning, a middle and an end: a starting dose, how far that titration can go up in terms of dosage and time interval, and a maximum, along with a clinical end point. Sometimes an order will fail to give a starting dose or a maximum dose. Another mistake is that the goal for titration may not be clear.”
Another frequent finding: When titrating two medications to the same goal—such as midazolam and propofol in concert for sedation—the order must state the same goal for each of the two medications. “I will sometimes see midazolam and propofol titration orders where each medication has a different goal, but they have to have the exact same expressed goal,” Ms. Sevcik said. “When you’re using two medications for the same purpose, that has to be stated in the order.”
Make your titration orders “followable,” she advised. “Many times, we tend to blame difficulties with following a titration order on nursing, when in fact it goes back to a faulty order. I recommend starting backward. Go and look at your titration medications, look at what the nursing staff is doing in actual practice, and create your orders based on that, as long as it is within the parameters of good, safe care.”
In such situations, “it’s fundamental that pharmacy, prescribers and nursing come together to create orders that nurses can actually follow, otherwise compliance with the order may be compromised,” she stressed. “Nurses should always report an order that is unclear and clarify before administration. It is best to simply start with a clear order.”
Compounding Conundrums
On the compounding side, Dr. Campbell cited the following compliance issues most commonly seen during site surveys:
- components of the compounding area not being cleaned per organization policy;
- areas of paint chipping on walls and ceilings;
- testing and certification of engineering controls not completed every six months; and
- HEPA filter testing not completed for secondary engineering controls during certification.
Other challenging areas for health systems included a lack of implementing organization policies and procedures—for example, proper hand hygiene, removal of jewelry in restricted areas and donning garb in alignment with organization policy.
Competency trends most commonly involved:
- incubators not maintained as required by the manufacturer;
- staff who conduct immediate-use compounding without having a documented competency;
- no documented competency for staff reading colony-forming unit counts of personnel or environmental testing;
- staff following USP <800> without training for handling hazardous medications identified by the organization; and
- staff with competency documentation gaps exceeding 12 months.
Dr. Campbell also reminded organizations that certain states, due to their own regulations, have delayed implementing <797> and <800> revisions. “We will evaluate your program based on your state’s standard,” he said. The Joint Commission extranet site contains links to preparation tools for a survey: one for organizations that will be evaluated against the revised chapters, and one for organizations that have delayed implementation of the revised chapters and instead reference the 2008 edition.
The sources reported no relevant financial disclosures.



This article is from the February 2025 print issue.