Originally published by our sister publication Specialty Pharmacy Continuum
The Department of Health and Human Services initiative, Ending the HIV Epidemic in the U.S., aims to slash new HIV infections by 90% by 2030. Experts in HIV care outlined how pharmacists can help reach this goal during a session at the ASHP Midyear 2024 Clinical Meeting & Exhibition, in New Orleans.
“In the U.S., we still have a ways to go to help end the HIV epidemic, and increasing PrEP [pre-exposure prophylaxis] uptake is one of the main strategies to doing this,” said Becks Wittenberg, PharmD, the senior infectious diseases specialty pharmacist at UC Davis Health, in Sacramento, Calif. “With our training, patient education, medication selection and monitoring, and laboratory assessment, pharmacists are poised to expand PrEP access and help close the HIV care gap.”
The main way that pharmacists can help expand PrEP use is by taking pressure off primary care providers (PCPs) to expand and administer treatment. Dr. Wittenberg outlined four steps that pharmacists can take to do this:
Forge Collaborative Practice Agreements
Pharmacist-led PrEP prescribing uses pharmacists’ knowledge of medications and expertise in patient education to efficiently step into the role of managing PrEP. This process often involves a collaborative practice agreement that defines the pharmacist’s scope and role in delivering care. At UC Davis Health, the agreement includes:

- providing initial patient education about PrEP options;
- using shared decision-making to identify the best regimen;
- prescribing PrEP;
- monitoring lab results, assessing continued clinical appropriateness, supporting patient adherence, mitigating side effects; and
- supporting discontinuation when appropriate.
“We tracked some data after the pilot of our pharmacist-led PrEP clinic and found that providers were eager to use our services to refer patients for PrEP,” Dr. Wittenberg said. “Our patient panel has grown over the years, and we have been able to provide a very high level of PrEP care to patients in our health system through this program.”
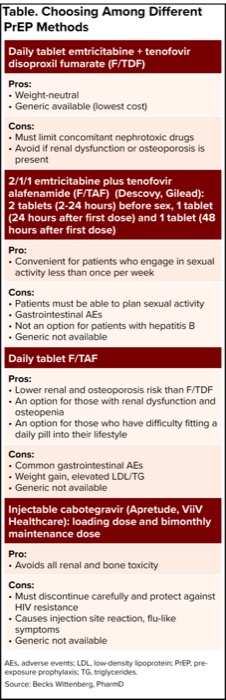
| Table. Choosing Among Different PrEP Methods |
| Daily tablet emtricitabine + tenofovir disoproxil fumarate (F/TDF) |
|---|
Pros:
|
Cons:
|
| 2/1/1 emtricitabine plus tenofovir alafenamide (F/TAF) (Descovy, Gilead): 2 tablets (2-24 hours) before sex, 1 tablet (24 hours after first dose) and 1 tablet (48 hours after first dose) |
Pro:
|
Cons:
|
| Daily tablet F/TAF |
Pros:
|
Cons:
|
| Injectable cabotegravir (Apretude, ViiV Healthcare): loading dose and bimonthly maintenance dose |
Pro:
|
Cons:
|
| AEs, adverse events; LDL, low-density lipoprotein; PrEP, pre-exposure prophylaxis; TG, triglycerides. Source: Becks Wittenberg, PharmD |
Focus on High-Risk Populations
The most recent CDC guidelines for administering PrEP recommend prescriptions for adults and adolescents who have an HIV-positive partner, a bacterial sexually transmitted infection (STI) in the past six months, a history of inconsistent or no condom use, or share drug injection equipment. Those at highest risk for HIV infection are young men who have sex with men (MSM). However, not all MSM are aware of PrEP and even fewer are on therapy. For example, according to CDC data presented by Dr. Wittenberg, 85% of MSM without HIV were aware of PrEP, but only 25% were on therapy. Pharmacists can help close this gap by screening for and engaging with those at higher risk for HIV infection, Dr. Wittenberg noted. A key tool in this effort is the use of sexual health questionnaires to identify patients who could benefit from PrEP, educating these patients and then offering therapy.
Determine Which PrEP Is Best
Before prescribing PrEP, pharmacists must screen for contraindicated medications, obtain a negative HIV test, and verify the absence of acute HIV symptoms. Pharmacists then need to decide which PrEP is best for each patient (Table). Pharmacists also must account for social and behavioral factors when deciding which treatment is best, including the fact that some patients may not have insurance coverage for the medication that best meets their needs.
Decide When to Involve the PCP
The final task for pharmacists providing PrEP is knowing when a patient should be brought back when they test positive for HIV or shows symptoms of an STI, Dr. Wittenberg noted. Other recheck reasons include rising serum creatinine with unclear cause or other abnormal labs with unclear etiology, or when a patient is unable to adhere to medication and required labs.
Ryan Tomlin, PharmD, a clinical HIV pharmacist at Trinity Health, in Grand Rapids, Mich., is part of a team that supports PCPs in PrEP management. For example, if a PCP at Trinity Health is not comfortable with prescribing PrEP, or simply doesn’t have appointment availability, “our pharmacist team can step in,” he said. “Our clinical pharmacists have all been training on PrEP and can offer the services described in Dr. Wittenberg’s presentation, including assessing eligibility, prescribing the medications, ordering and monitoring labs, educating over risk reduction, and performing follow-up visits.”
Dr. Tomlin emphasized the importance of interdisciplinary collaboration in expanding PrEP. Doctors, nurses and social workers support pharmacists by treating medical complications, managing testing, and solving social and behavioral challenges.
Dr. Wittenberg agreed that collaborative practice is crucial for PrEP expansion to be successful. “When pharmacists are flexible and creative in our outreach, and utilize wraparound care with a multidisciplinary team, we have a much better chance of offering a larger patient group PrEP and retaining them in care.”
The sources reported no relevant financial disclosures.